FDA Expands Use of Spinal Cord Stimulators to More Types of Back Pain
/By Pat Anson, PNN Editor
The U.S. Food and Drug Administration continues to expand the use of spinal cord stimulators, despite a growing body of research that questions the safety and effectiveness of the devices.
This month the FDA approved the use of Abbott’s spinal cord stimulators for the treatment of chronic back pain in people who are unable to get corrective surgery – known as non-surgical back pain -- because they are too medically frail or have numerous degenerative disc problems. Those patients are usually treated with pain medication, physical therapy or spinal injections.
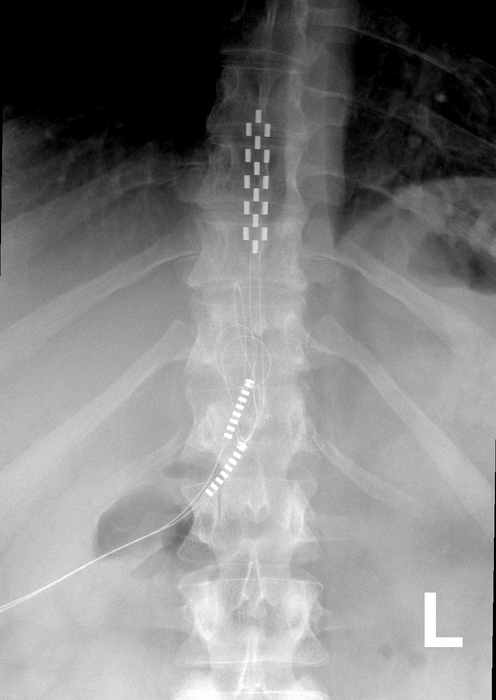
FDA approval was granted after a clinical study showed that SCS devices equipped with Abbott's BurstDR technology provided significant pain relief, better physical function, and improved quality of life in 200 patients with non-surgical back pain. The devices are surgically placed near the spine and emit mild electrical impulses to disrupt pain signals before they reach the brain.
Participants in the study had chronic and disabling back pain for an average of nearly 13 years before getting the devices.
"We have struggled with how to treat people who weren't considered a good surgical candidate because we didn't have clear, data-driven treatment options for non-surgical back pain," Timothy Deer, MD, CEO of the Spine and Nerve Centers of the Virginias, said in an Abbott press release. "This new indication for Abbott's SCS devices, together with BurstDR stimulation, allows physicians the ability to identify and treat a new group of people, providing them with relief from chronic back pain."
BurstDR stimulation uses mild electrical pulses — or bursts — without creating an uncomfortable tingling sensation in the spine known as paresthesia. All of Abbott's SCS devices use BurstDR technology.
Nine out of ten patients who received BurstDR therapy experienced significantly better function or pain relief, with pain levels reduced an average of nearly 70 percent. The improvements were sustained 12 months after the devices were implanted.
"This FDA expanded indication approval for our SCS devices is a significant step forward in Abbott's goal to provide treatment access to those who suffer daily with chronic back pain but are not eligible for corrective surgery," said Pedro Malha, vice president of neuromodulation for Abbott.
SCS devices were long considered a treatment of last resort for people with severe back, neck and leg pain, but in recent years the FDA has expanded use of the devices for conditions such as painful diabetic neuropathy. The devices are often promoted as safer alternatives than opioid pain medication.
Recent research, however, has raised questions about the safety, efficacy and long-term benefits of the devices. A recent Cochrane review concluded the stimulators work no better than a placebo for treating chronic low back pain, and provide little or no improvement in quality of life. In a review of 13 clinical trials, researchers found little clinical data on the long-term effectiveness of SCSs, and noted that most of the studies lasted less than a month, were poorly blinded, or funded by device makers.
A 2018 study by investigative journalists found that SCSs have some of the worst safety records of medical devices tracked by the FDA.
A 2020 FDA review of adverse events involving stimulators found that nearly a third were reports of unsatisfactory pain relief. Other common adverse events are nerve damage, infections, and device malfunctions that may lead to further surgeries.
A 2022 study found that patients who get the devices did not reduce their use of opioids, and continued getting medical procedures such as injections, epidurals and radiofrequency ablation.