‘I’m Still in Pain’: A Patient’s Long Wait to See a Specialist
/By Molly Castle Work, KFF Health News
Teresa Johnson can’t escape the pain. It’s as if she’s getting pierced by needles all over her body, all at once. At night, she sometimes jolts out of sleep thinking bedbugs are attacking her. But it’s just the unfailing pain — day in and day out.
Johnson, 58, said her ordeal started in September 2022, when she went for a CT scan of her abdomen after a bout of covid-19. Though Johnson warned the lab she was allergic to iodine, she believes the lab tech used it in an injection, triggering an allergic reaction. She spent the next three weeks in the hospital, feeling as if her body was on fire.
When she was discharged to her home at the base of the San Jacinto Mountains in Riverside County, Johnson said, her quality of life deteriorated and her frustration mounted as she waited for her Medi-Cal plan to get her assessed by a specialist. She could barely walk or stand, she could no longer cook for herself, and sometimes she couldn’t even lift her leg high enough to step into the tub.
“I would never wish this on anybody,” Johnson said while rocking back and forth on the couch to still the pain. “You don’t know if you should cry, or just say OK, I can make it through this. It messes with you mentally.”
Johnson said her primary care doctor told her he wasn’t sure what triggered the pain but suspects it was compounded by the lingering effects of covid.
Johnson, who is diabetic, developed neuropathy, a type of nerve damage, possibly after the allergic reaction caused her blood sugar levels to skyrocket, her doctor told her.
He referred Johnson, who receives care through California’s Medicaid program for low-income people, to an endocrinologist in March.
But Johnson said she was not offered timely appointments, and it took more than six months, four referrals, multiple complaints to her health plan, and a legal aid group’s help to finally snag a phone call with an endocrinologist in mid-September.

TERESA JOHNSON
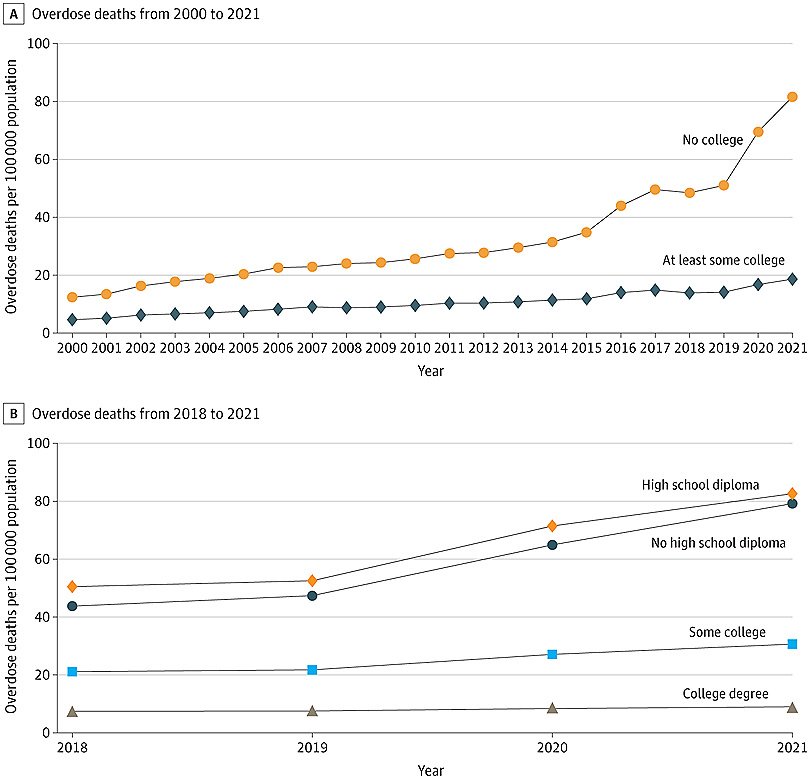
Access to specialists — from gastroenterologists to cardiologists — has been a long-standing challenge for many Medi-Cal patients, especially those in rural areas or regions facing staff shortages. The Inland Empire, where Johnson lives, has the second-lowest supply of specialists in the state, according to the California Health Care Foundation.
The state Department of Managed Health Care, which regulates most Medi-Cal health plans, requires plans to get patients in to see specialists within 15 business days, unless a longer waiting time would not harm the patient’s health. But the timeline often looks very different in reality.
“It’s hard to get a specialist to contract for Medi-Cal patients. Period,” said Amanda Simmons, executive vice president of Integrated Health Partners of Southern California, a nonprofit organization that represents community health clinics. “Specialists don’t want to do it because reimbursement rates are so low.”
Johnson said she made her first call in March to the endocrinologist assigned by her Medi-Cal insurer, Inland Empire Health Plan, and that the office offered her an appointment several months out. Over the next four months, she received three more referrals, but she said she got a similar response each time she called. When Johnson objected to the lengthy wait times, requesting earlier appointments, she was told there was no availability and that her condition wasn’t urgent.
“They told me it wasn’t important,” Johnson said. “And I asked, ‘How would you know? You’ve never seen me.’”
Esther Iverson, director of provider communications for the plan, declined to speak about Johnson’s case but said the plan makes every effort to meet the 15-day requirement. It can be challenging to meet the standard, she said, due to a lack of available physicians — especially for certain specialties, such as endocrinology and pain management.
She pointed to the nationwide physician shortage, which is more pronounced in rural areas, including parts of San Bernardino and Riverside counties, where the plan operates. She also noted that many physicians decided to leave the field or retire early due to burnout from the covid pandemic.
At the same time, she said, the plan’s enrollment ballooned to 1.6 million as eligibility expanded in recent years. Statewide, more than 15 million Californians are enrolled in Medi-Cal.
“The highest priority for us is timely access to quality care,” Iverson said.
‘I’m So Burned Out’
During her quest, Johnson enlisted the help of Inland Counties Legal Services, which provides free legal representation to low-income residents. They called the plan multiple times to request earlier appointments but got mired in bureaucratic delays and waiting periods.
In one instance in August, after the insurer told Johnson it couldn’t meet the 15-day time frame, her legal representative, Mariane Gantino, filed an appeal, arguing that Johnson’s request was urgent. The insurer’s medical director responded within a few hours denying the claim, saying the plan concluded that her case was not urgent and that a delay would not cause a serious threat to her health.
“I’m so burned out after dealing with this for so long,” Johnson said in mid-September. “Why do they have the 15-day law if there aren’t going to be any consequences?”
A few days later, Johnson finally received the call she had been waiting for: an offer of a phone appointment with an endocrinologist, on Sept. 18. During the appointment, the doctor adjusted her diabetes and other medications but didn’t directly address her pain, she said.
“I’m in the same position,” Johnson said. “I’m still in pain. What’s next?”
Over the years, Johnson has worked a variety of jobs — from driving eighteen-wheelers cross-country to weaving hair — but her most consistent work was as a caregiver, including to her six children, 21 grandchildren, and three great-grandkids, with another great-grandchild on the way. Now, because of her extreme pain, the roles have been reversed. A daughter and granddaughter who live with her have become her full-time caregivers.
“I can’t do nothing. I can’t take care of my grandkids like I used to,” said Johnson, who sleeps most of the day and wakes up only when her pain medication wears off. “I was planning to take care of the new baby that’s coming. I probably can’t even hold her now.”
This article was produced by KFF Health News, which publishes California Healthline, an editorially independent service of the California Health Care Foundation.